Stop Guessing. Get your 2026 Rate in 60 Seconds via Phone.
Navigate the marketplace with confidence. Find the subsidies you deserve in under 2 minutes.
• ACA / Marketplace Compliant
• $0 Premiums Available
• No Waiting periods
Stop Guessing. Get your 2026 Rate in 60 Seconds via Phone.
Navigate the marketplace with confidence. Find the subsidies you deserve in under 2 minutes.
• ACA / Marketplace Compliant
• $0 Premiums Available
• No Waiting periods
Affordable Coverage
Thanks to the ACA, 4 out of 5 Americans qualify for plans under $10/mo. See if you qualify for a $0 premium
Full Major Medical Coverage
You cannot be denied coverage due to pre-existing conditions. No health questions asked. Guaranteed acceptance.
Full Major Medical Coverage
All ACA plans must cover the 10 Essential Health Benefits: Prescriptions, ER visits, Maternity, and Preventive Care
Affordable Coverage
Thanks to the ACA, 4 out of 5 Americans qualify for plans under $10/mo. See if you qualify for a $0 premium.
No Waiting Periods
You cannot be denied coverage due to pre-existing conditions. No health questions asked. Guaranteed acceptance.
Full Major Medical
All ACA plans must cover the 10 Essential Health Benefits: Prescriptions, ER visits, Maternity, and Preventive Care.
WE WORK WITH TOP RATED CARRIERS







WE WORK WITH TOP RATED CARRIERS

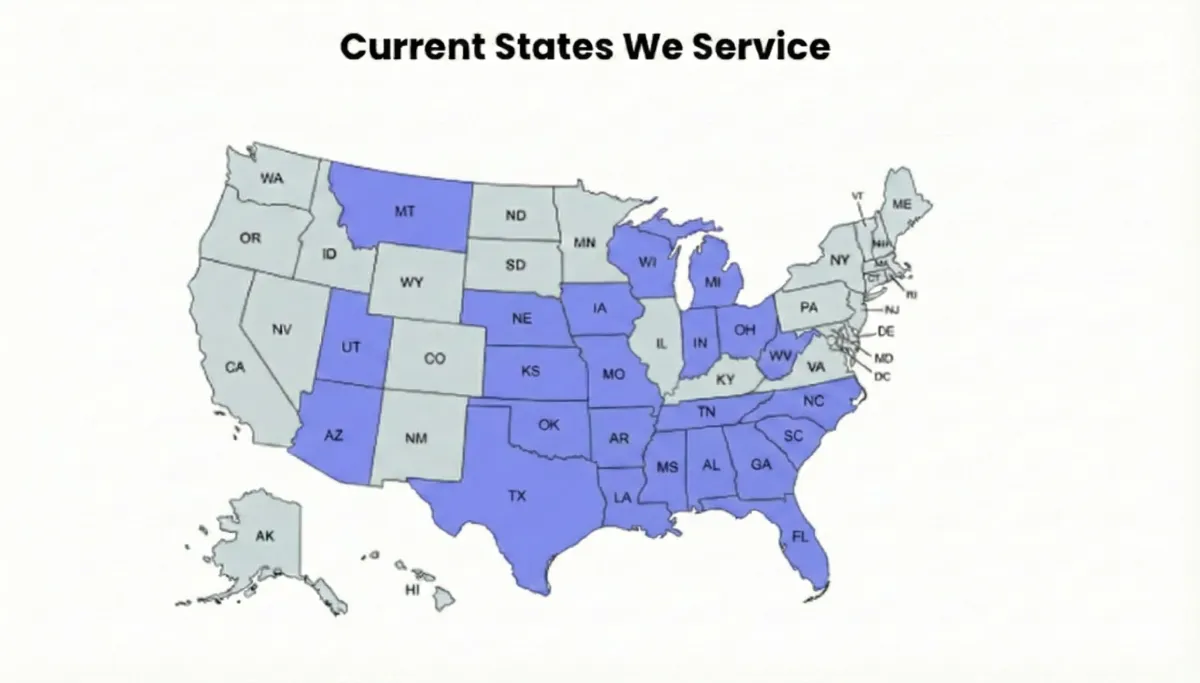
Licensed Experts Serving Your Community.
"We are currently licensed to serve families in 28 states across the US, including:" FL, GA, AL, SC, NC, TN, MS, LA, TX, OK, MO, AR, KS, AZ, NE, IA, UT, MT, WI, IN, OH, MI, WV
2026 Empathy Insurance Advisors. All Rights Reserved. | NPN: 19291077
Not a Government Agency: This website is an independent digital media & advertising publisher. This website is not a federal or state Marketplace website and is not affiliated with the Affordable Care Act (ACA) or any government entity.
Availability: We do not offer every plan available in your area. Any information we provide is limited to those plans we do offer in your area. Please contact Healthcare.gov or your local State Marketplace to get information on all of your options.
TCPA Consent: By clicking the button above, you consent to receive marketing calls, text messages, and emails from a licensed insurance agent at the number provided, including through the use of an automated dialing system. Consent is not a condition of purchase. Message and data rates may apply.